Hair loss in women is rarely just one thing. Most women who notice thinning or shedding have been told it’s “stress” or “hormones”, which isn’t wrong, but it’s not the full picture either. The reality is that several physiological factors tend to overlap, and unless you look at all of them together, it’s easy to miss what’s actually driving the problem.
Here’s where it gets interesting: the body often signals these imbalances through the hair long before other symptoms become obvious.
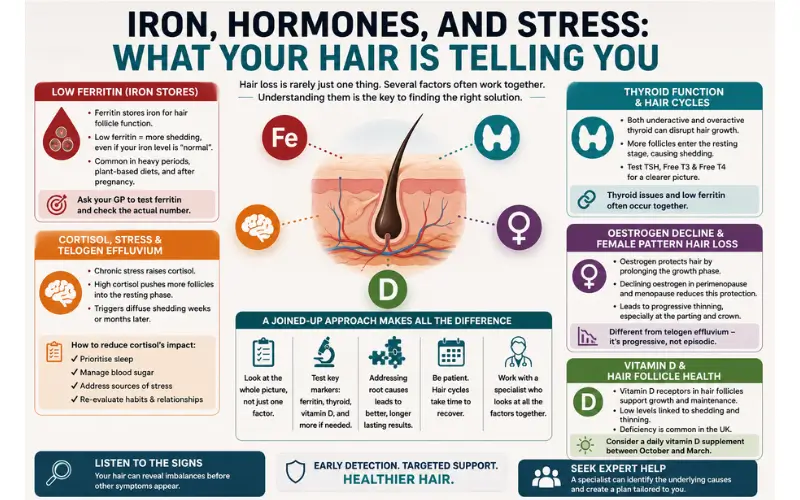
Why Ferritin Matters More Than Your Iron Count
One of the most commonly overlooked causes of female hair loss is low ferritin, the protein that stores iron in the body. Standard blood panels will often come back “normal” for iron, even when ferritin is low enough to affect hair growth. That’s because ferritin is a separate marker, and many GPs don’t test for it automatically.
Hair follicles are metabolically active. They need ferritin to function properly, and when stores drop too low, the body prioritises more critical functions and redirects resources away from hair production. The result is usually a diffuse shedding pattern, with hair thinning all over rather than in one specific area. Women who have heavy periods, follow a plant-based diet, or have had recent pregnancies are particularly at risk of ferritin depletion.
If you’re experiencing unexplained shedding, it’s worth asking your GP to test ferritin specifically and to request the actual number, not just a pass or fail result. Ferritin levels considered “normal” for general health can still be too low to support healthy hair growth.
Thyroid Function and Hair Cycles
Both an underactive and an overactive thyroid can disrupt the hair growth cycle. The thyroid regulates metabolism throughout the body, and hair follicles are directly sensitive to thyroid hormones. When levels are off, the hair cycle is pushed out of phase, and more follicles shift into the resting stage at once, leading to increased shedding several months later.
This is where women often get confused. Because the shedding happens weeks or even months after the hormonal disruption, it’s not always easy to connect the two. A basic thyroid panel, including TSH, Free T3, and Free T4, will give a clearer picture than TSH alone.
It’s also worth noting that thyroid issues and low ferritin frequently occur together, particularly in women of reproductive age and those in perimenopause.
Cortisol, Stress, and Telogen Effluvium
Chronic stress raises cortisol levels, and sustained high cortisol is one of the most direct pathways to a condition called telogen effluvium, a form of diffuse hair shedding triggered when a significant number of follicles are pushed into the resting phase simultaneously. This can happen after a major life event, illness, surgery, or simply months of sustained psychological pressure.
This is something that comes up regularly in hair loss consultations, where female patients often present with several overlapping factors, not just one clear cause. If these signs sound familiar to you, you might benefit from talking to a specialist at a reputable UK clinic, like Treatment Rooms London. They will take into consideration all of your symptoms and advise you on the best way forward.
What makes it harder to manage is that cortisol also suppresses thyroid function and can affect iron absorption, so these systems don’t operate in isolation. Practical steps to reduce cortisol’s impact on hair include:
- Prioritising sleep
- Managing blood sugar levels through regular meals
- Addressing the sources of stress where possible
- Re-evaluating your habits and relationships to find the most likely culprits
These aren’t quick fixes, but they do remove the physiological conditions that prolong shedding.
Oestrogen Decline and Female Pattern Hair Loss
As women enter perimenopause and menopause, oestrogen levels fall. Oestrogen plays a protective role for hair. It prolongs the growth phase of the hair cycle and helps offset the effects of androgens like DHT, which can miniaturise hair follicles over time. When oestrogen drops, that protective buffer reduces, and many women begin to notice thinning, particularly along the parting and at the crown.
This is distinct from telogen effluvium in that it tends to be progressive rather than episodic. It’s also the stage at which female pattern hair loss becomes more visible, and it often coincides with other hormonal changes that further complicate the picture.
Vitamin D and Its Role in Hair Follicle Health
Vitamin D is another factor that deserves attention, particularly in the UK where sunlight exposure is limited for much of the year. Hair follicles contain vitamin D receptors, and research has linked low levels of the vitamin to both telogen effluvium and female pattern hair loss. Vitamin D plays a part in the creation of new hair follicles and helps maintain the ones you already have, so a deficiency can slow the growth cycle and contribute to overall thinning.
What makes this relevant to the broader picture is that vitamin D deficiency often appears alongside low ferritin and thyroid dysfunction. It is one of those markers that can quietly sit below optimal levels for months or years without being flagged, especially if your GP hasn’t included it in routine bloodwork.
A simple blood test can confirm where you stand, and supplementation through the autumn and winter months is a straightforward step that many women find helpful. The NHS recommends that adults in the UK consider taking a daily vitamin D supplement between October and March, which is worth bearing in mind if your hair tends to shed more heavily during the colder months.
Why a Joined-Up Approach Makes All the Difference
One of the biggest frustrations women face when dealing with hair loss is being given a single explanation when the cause is almost always multifactorial. A GP might identify low ferritin but not check thyroid function. A dermatologist might diagnose female pattern hair loss but not explore whether chronic stress or nutritional gaps are accelerating the process.
This is why women who seek help from a specialist with experience in female hair loss tend to get better outcomes. A thorough initial assessment that covers bloodwork, medical history, lifestyle and hormonal status gives a much clearer foundation for treatment than any single test in isolation.
Closing Remarks
Most cases of female hair loss have more than one contributing factor. Getting a clear answer usually means looking at ferritin, thyroid function, cortisol, and hormonal changes together, ideally with a clinician who specialises in hair.
Treating one factor in isolation can bring limited results if the others are left unaddressed. The more you understand about what’s happening internally, the better placed you’ll be to decide on next steps.


